SYSTEMIC SCLEROSIS (SSc)
Systemic Sclerosis (SSc) is a systemic autoimmune rheumatic disease. SSc is characterised by excess production and accumulation of collagen, cause fibrosis in the skin and internal organs and by injuries to small arteries.
The pathogenesis of this disease is not fully understood.
SYSTEMIC SCLERODERMA: HISTORICAL ORIGINS
In 400 BC, first report of scleroderma found, when Hippocrates noted “thickening of the skin” in some patients. The first detailed description was made by Carlo Curzio in 1753, who observed hard, wood-like skin in a young woman.
In 1836, Giovambattista Fantonetti introduced the term “scleroderma,” derived from the Greek words sclero (hard) and derma (skin), to describe generalized skin hardening.
Related article:
Understanding Multiple Sclerosis: An Autoimmune Attack on CNS
SYSTEMIC SCLEROSIS RISK FACTORS
The exact cause of SSc is unknown, but current evidence suggests that the disease may be triggered by environmental exposures (such as toxins or chemicals), viral infections, microbial pathogens, or other still not identified mechanisms.
Environmental exposures
Research suggests that both environmental and viral factors may contribute to the development of SSc. Certain environmental exposures such as polyvinyl chloride, contaminated rapeseed oil (associated with Spanish toxic oil syndrome).
L-tryptophan containing products (linked to eosinophilia–myalgia syndrome), silica dust, organic solvents, toluene, xylene, trichloroethylene and gadolinium (associated with nephrogenic systemic fibrosis) have been shown to cause fibrotic conditions that resemble SSc, supporting the possibility of an environmental trigger.
In addition, the presence of an early type I interferon signature and activation of Toll-like receptor 8 (TLR8) by Epstein–Barr virus (EBV) genes in monocytes from patients with SSc suggest a potential viral contribution to disease pathogenesis. Other microorganisms such as cytomegalovirus (CMV), parvovirus B19 also cause SSc.
Age Factor
SSc most commonly affects adults between the ages of 30 and 50, however, it can occur at any age (children and old age).
Genetic factor
SSc is not a genetic disease but genetic factors play crucial role in development of SSc.
Vascular alterations
Vascular disturbance also plays important role in development of SSc. In SSc blood vessels damage and leads to serious condition such as:
- Raynaud’s Phenomenon (Fingers or toes turn white/blue in cold or stress due to reduced blood flow),
- Small artery vasculopathy (Damage and narrowing of small blood vessels),
- Digital ulcers (Painful sores on fingers or toes due to poor circulation),
- Telangiectasias (Small, visible, dilated blood vessels on the skin or mucous membranes) in various internal organs.
Blood vessels can affect internal organs, disturb their function and potentially lead to organ failure in severe cases.
Scleroderma Types
Scleroderma classified into two types:
- Localized scleroderma (LoSc)
- Systemic scleroderma (SSc), SSC present in two forms: limited and diffuse.
Localized Scleroderma (LoSc)
LoSc affects skin lesions and can occur in various forms, the most important of which are:
- Plaque morphea (PMLoSc)— In PMLoSc, lesions occur in the form of plaques that appear on a limited part of the body specially in the trunk area.
- Generalized (GLoSc)— In GLoSc, lesions are large and much diffuse usually four or more foci in the size of >3 cm in diameter. It involves multiple parts of the body at least two anatomical sites.
- Linear form (LLoSc) — In LLoSc, the lesion appears as a linear or band-like area of thickened, indurated skin, most commonly affecting the upper or lower limbs. It typically follows the lines of Blaschko.
- Linear form “en coup de sabre” (LLoSceCS; ECDS) — In this variant, lesions typically occur on the scalp and/or forehead and appear as a linear, depressed, scar-like band resembling a strike from a saber.
Systemic scleroderma (SSc)
The most characteristics symptoms are presence of skin lesions. In SSc skin loses its elasticity, feel tight and tense that gradually develops into thickened and hardened.
SSc is not limited to only skin but affects whole body (multiple organs) such as lungs, kidney, and heart. However, the severity and distribution of skin changes vary between patients. Based on how extensive the skin involvement is, SSc is classified into:
- Limited systemic scleroderma (lSSc)
- Diffuse systemic scleroderma (dSSc)
Limited systemic scleroderma (lSSc)
lSSc is characterized by the early onset of Raynaud’s phenomenon. Skin involvement is restricted to the hands, forearms, feet, and face. The disease may also cause fibrotic lesions in the gastrointestinal tract, leading to difficulty in swallowing and acid reflux. In addition, fibrotic lesions of the lungs can occur, resulting in breathing problems.
Diffuse systemic scleroderma (dSSc)
dSSC is a more aggressive form of systemic sclerosis in which Raynaud’s phenomenon occurs along with skin thickening. Unlike the limited form, skin involvement is not restricted to the hands, forearms, feet, and face but spread beyond the elbows and may involve the trunk (chest and abdomen). dSSc is also severely affects internal organs, including the gastrointestinal tract, lungs, heart, and kidneys.
HOW SYSTEMIC SCLEROSIS AFFECTS DIFFERENT ORGANS
Skin involvement
Skin thickening in SSc typically starts at the tips of the fingers and toes and gradually spreads inward toward the body, but the severity and progression vary widely between patient to patient.
Skin thickening occurs in three phases-
- Puffy finger phase
- Prolonged fibrotic phase
- Skin-softening phase
1. Puffy finger phase
In initial phase, hand fingers become puffy due to inflammation in very small blood vessels (capillaries, arterioles, venules). This causes non-pitting edema especially in the fingers and hands. Patients may experience itching, pain and feeling of tightness.
A very common and characteristic feature during this stage is Raynaud’s phenomenon.
2. Prolonged fibrotic phase
This is the second phase during which skin of finger become hard and thick, condition known as sclerodactyly. Sclerodactyly starts from the knuckle joints (metacarpophalangeal joints). Progressive hardening and thickening of skin lead to ulcer, scar and bacterial infections of the fingertips.
At this stage, hardening and thickening starts spreading facial skin that leads to small visible dilated blood vessels, also called spider veins (telangiectasias), nose deformity, microstomia (abnormally small mouth) and wrinkles radiating around the mouth (Radial furrows). Because of skin thickening and tightening, the face may lose normal expressions that condition known as ‘mask image’.
3. Skin-softening phase
It is the last and final phase in systemic sclerosis (SSc). In this phase, outer layers of the skin may gradually become softer and skin regain its normal skin texture and flexibility. However, the deeper (subcutaneous) layers remain permanently damaged. These deeper tissues are already replaced by fibrotic (scar-like) tissue. So, even if the surface feels softer, the underlying fibrosis does not fully reverse.
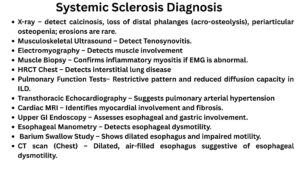
Diagnosis methods to detect skin involvement
- Rodnan Skin Score (mRSS)
- Ultrasound
- Durometry
- Optical Coherence Elastography (OCE)
SSc affect blood vessels
In patients, skin lesions associated with damage in small blood vessels. Over the years, doctors identified characteristics ‘scleroderma pattern’, which is include the presence of giant capillaries (with an apical diameter ≥ 50 μm) or the presence of abnormal vessel with a smaller number of capillaries.
Diagnosis method to detect blood vessels involvement
- X-ray and ultrasound
- Ultrasound shear wave elastography (US-SWE)
- Color Doppler ultrasound
- Magnetic resonance imaging (MRI)
SSc affect gastrointestinal tract area
It is more common about 90% patients have issue related with gastrointestinal tract area with lesions. SSc affect the entire gastrointestinal tract (GIT), from the mouth to anus. Patients may have issue with oral lesions, and may develop esophageal dysphagia (difficulty swallowing).
SSc in upper gastrointestinal tract cause microstomia, xerostomia (decreased saliva secretion), taste disorders, periodontium and taste buds, dysphagia, lower esophageal sphincter (LOS) abnormalities, gastroesophageal reflux disease (GERD), Barrett’s esophagus, and esophageal adenocarcinoma.
Gastric antral vascular ectasia (GAVE) is characteristic feature of SSc with GIT involvement. In GAVE, lesions, can lead to acute or chronic gastrointestinal bleeding. During diagnosis, this lesion appears red longitudinal bands arranged along the folds of the stomach, extending toward the pylorus, that condition known as ‘watermelon stomach’.
In systemic sclerosis, patients may develop chronic intestinal pseudo-obstruction (CIPO), that cause intestinal motility disorders, results in chronic nausea, abdominal pain, bloating, and constipation.
Impaired motility can also lead to small intestinal bacterial overgrowth (SIBO), resulting in bloating, abdominal pain, diarrhoea, and malabsorption.
SSc affect lungs
These two conditions are the most common respiratory complications in SSc.
Systemic scleroderma-associated interstitial lung disease (SSc-ILD): In SSc, respiratory system inflamed and fibrotic that cause stiffness and reduction in oxygen exchange, leads to systemic scleroderma-associated interstitial lung disease (SSc-ILD).
Pulmonary arterial hypertension (PAH): Due to narrowing and remodeling of small pulmonary blood vessels, there is high blood pressure in lung arteries known as pulmonary arterial hypertension (PAH).
Some patients develop cylindrical bronchiectasis, which is a permanent and progressive widening of the bronchi (airways). Because the bronchial walls are damaged, they lose their normal shape and elasticity, leading to chronic cough and mucus accumulation.
There are also reports of damage to small lung blood vessels (pulmonary capillaries). This can cause diffuse alveolar hemorrhage (DAH), a serious condition in which bleeding occurs into the air sacs (alveoli) of the lungs.
Some patients may develop pleuritis, which is inflammation of the pleura (the membrane surrounding the lungs). This can lead to lymphocytic effusion, meaning fluid rich in lymphocytes (a type of immune cell) accumulates around the lungs.
Diagnosis to detect lung involvement
- Ultrasonography
- High-resolution computed tomography (HRCT)
SSc affect heart
Evidence suggests that in SSc, approximately 27% of deaths are due to heart diseases. Most common heart disease are myocarditis, coronary artery disease, myocardial fibrosis, conduction system abnormalities, valvular regurgitation, heart failure, or pericardial and/or endocardial disease.
In systemic sclerosis (SSc), heart lesions develop slowly and silently.
In the first or initial phase, there is issue with cardiac function and blood vessels abnormalities, but patients usually have no symptoms, and these changes may still be reversible. Over time, the small coronary arteries (which supply blood to the heart muscle) cause reduced blood and affect the myocardium.
Because of poor blood supply, Local ischemia (reduced oxygen delivery) occurs. This leads to myocardial fibrosis (scarring of heart muscle). As fibrosis increases, stiffness in heart muscle increase and ventricles become thick. Both diastolic dysfunction and systolic dysfunction develop and arrhythmias (abnormal heart rhythms) may occur. SSc patients also develop Myocardial edema (swelling of heart muscle).
SSc affect Kidney area
In systemic sclerosis (SSc), heart and lung involvement is often associated with kidney problems. Kidney damage may develop faster than lung damage because the kidneys normally work under higher blood pressure. Over time, the small blood vessels in the kidneys become thickened and scarred, which damages the filtering units called glomeruli. As a result, kidney function gradually decreases.
About 50% of patients show abnormal urine or blood test results, such as protein in the urine, reduced kidney filtration (low GFR), increased creatinine levels, or high blood pressure. In severe cases, a serious complication called scleroderma renal crisis (SRC) can occur, which involves sudden severe high blood pressure and rapid kidney failure.
Read article:
Lung Cancer: Causes, Symptoms & Treatment
Adenomyosis: Signs, Risk Factors, and Best Treatment Options