WHAT IS LUPUS?
Lupus is chronic inflammatory autoimmune disease. It can affect many parts of the body such as kidney, liver, hear, lungs and brain.
Lupus cause inflammation in different organs because the immune system becomes dysregulated and starts attacking its own body tissues.
People with lupus experience periods when symptoms suddenly worsen, known as flares, with pain that may range from mild to severe, followed by periods when they feel little or no pain.
In lupus, the immune system fails to recognize self-cells and starts attacking healthy tissues. It produces autoantibodies, which combine with other immune proteins to form immune complexes that damage normal tissues. This reflects a loss of self-tolerance due to abnormal immune function, leading to chronic inflammation and tissue injury.
Treatment for lupus is individualized and may include medications, lifestyle modifications, and supportive care to control symptoms, reduce disease activity, and improve quality of life.
Related article:
Gout: Causes, Symptoms, Pseudogout and Risk Factors
Rheumatoid Arthritis (RA): Symptoms, Causes & Risk Factors
LUPUS CLASSIFIED INTO FOUR MAIN TYPES:
- Neonatal and pediatric Lupus Erythematosus (NLE)
- Discoid Lupus Erythematosus (DLE)
- Drug Induced lupus (DIL)
- Systemic lupus erythematosus (SLE)
1. Neonatal and pediatric lupus erythematosus (NLE)
Neonatal lupus erythematosus (NLE) is a rare form of lupus found in newborns.
It is believed to occur when maternal autoantibodies cross the placenta and affect the infant. Although many infants are exposed to their mother’s autoantibodies, only about 1% develop NLE.
NLE commonly affects the heart, liver, and skin.
When the heart is involved, NLE can cause severe illness or even death. However, in most infants with involvement of other organs, such as the liver or skin, symptoms often improve or resolve spontaneously within a few months.
2. Discoid lupus erythematosus (DLE)
Discoid lupus erythematosus (DLE) causes chronic scarring and skin atrophy (thinning) and is worsened by sunlight. The skin becomes photosensitive, and the disease mainly affects the face, scalp, and ears.
Some patients with DLE may later develop systemic lupus erythematosus (SLE), which affects multiple organs, or DLE may already be present in patients with SLE.
The cause of DLE is believed to be genetic, and the condition is more common in women. African American women between 20 and 40 years of age are at higher risk of developing DLE.
Treatment for DLE includes chemical and physical sunscreens, topical corticosteroids, and antimalarial drugs to prevent disease flares.
Diagnosis is often made by biopsy of skin lesions, typically from the scalp, face, neck, or arms.
3. Drug induced lupus (DIL)
Drug-induced lupus (DIL) develops when exposure to certain medications triggers the immune system to mistakenly attack the body’s own tissues. This autoimmune reaction may affect multiple organ systems, including the joints, skin, and muscles.
Unlike systemic lupus erythematosus, the symptoms of DIL usually improve and resolve after the offending drug is discontinued.
4. Systemic lupus erythematosus (SLE)
Systemic lupus erythematosus (SLE) is the most common type of lupus and is often simply called lupus. It differs from other forms of lupus because it can affect multiple organ systems.
SLE is more common in women of childbearing age, although it can affect both men and women at any age. It is more frequently found in African Americans, Asians, Hispanics, and Native Americans.
SLE IS AUTOIMMUNE DISEASE
B cells Overactivation
In SLE, B cells become abnormally overactive after being stimulated by T cells and self-antigens. This leads to the excessive production of autoantibodies directed against antigens found on apoptotic (dying) cells.
Defective disposal of Apoptotic cell
Normally, apoptotic cells are quickly and efficiently removed. In SLE, however, this clearance process is defective. During cell death, fragments of cellular material move to the surface of the dying cell, exposing antigens that are normally hidden inside the cell. Examples of these antigens include nucleosomes and anionic phospholipids, which can trigger an immune response.
Because phagocytic cells function poorly, apoptotic cells are not properly cleared. As a result, these exposed antigens persist and are recognized by the immune system, leading to continued activation of T cells and B cells.
How B cell activated?
SLE is thought to begin when a T- cell interacts with an antigen-presenting cell (APC) displaying these self-antigens. The T-cell receptor binds to the antigen–MHC complex on the APC, causing cytokine release, inflammation, and activation of B cells.
Activated B cells then proliferate and produce IgG autoantibodies, which can damage tissues by forming immune complexes.
Unlike in healthy individuals, self-reactive T cells and B cells are not adequately controlled in SLE. They interact with each other and continue producing pathogenic autoantibodies, sustaining chronic inflammation and autoimmune tissue damage.
Many of the autoantibodies produced are antinuclear antibodies (ANAs). These antibodies are directed against components within the cell nucleus, such as DNA, RNA, and nuclear proteins.
Testing for ANAs is a key part of diagnosing SLE, because most patients with SLE have detectable ANAs in their blood. Additionally, a single patient may have more than one type of ANA, meaning multiple nuclear targets can be attacked at the same time.
SLE RISK FACTORS
Exact reason behind SLE is unknown, but there are genetic, hormonal and environmental factors as well as immune abnormalities have been reported.
SLE in identical and fraternal twins
Studies shows that genes play an important role in SLE. Identical twins, who share the same genes, are much more likely to both have SLE than fraternal twins, who share fewer genes.
Environmental Factors
Environmental factors can trigger or worsen SLE.
Ultraviolet (UV) light
One important factor is ultraviolet (UV) light, which stimulates keratinocytes in the skin. This activation can lead to B-cell stimulation and autoantibody production and may also increase T-cell activity, further enhancing autoantibody formation.
Viral infections
Certain viral infections, particularly Epstein–Barr virus (EBV), have been associated with the development of SLE, especially in children. Patients with SLE often show higher antibody levels (titers) against EBV, suggesting prior immune activation.
Other factors
Other environmental exposures, such as cigarette smoking, silica dust, and some hair products (including dyes), are also considered potential triggers that may initiate or exacerbate lupus in susceptible individuals.
Sex and Age
SLE occurs more frequently in women, especially those of childbearing age. It is thought that SLE is related to hormonal factors, particularly estrogen. Research shows that women who use oral contraceptive or other hormonal therapies are more prone to developing SLE.
In contrast, men have a lower risk, similar to that seen in prepubertal girls and postmenopausal women, groups with lower estrogen levels.
Klinefelter’s syndrome
Evidence supporting that Klinefelter’s syndrome, a condition in which males have an extra X chromosome and show a higher incidence of SLE, support the link between hormones (and possibly X-chromosome–related factors) and SLE development.
SLE SYMPTOMS
SLE presents with a wide range of general and organ-specific symptoms.
General symptoms include fever, fatigue, and weight loss.
The skin, musculoskeletal system, and lungs are most commonly affected.
Skin involvement often appears as a red rash over the nose and cheeks after sun exposure, known as the butterfly (malar) rash. Photosensitivity may also cause rashes on other sun-exposed areas. Other skin symptoms include hair loss (alopecia), Raynaud’s phenomenon, and mouth or nasal ulcers.
Musculoskeletal symptoms include joint pain (arthralgia), muscle pain (myalgia), and arthritis, which can affect both small and large joints and typically causes pain, stiffness, and inflammation.
Pulmonary involvement may cause painful breathing, cough, and shortness of breath, with conditions such as pleural effusion and pulmonary hypertension.
SLE can also involve multiple other organ systems:
Cardiovascular system: pericarditis, myocarditis, endocarditis, and coronary artery disease. Some treatments (e.g., corticosteroids and immunosuppressants), along with traditional risk factors, may increase cardiovascular risk.
Gastrointestinal system: nausea, vomiting, and abdominal pain.
Hematological system: anemia, leukopenia, and thrombocytopenia. Antiphospholipid antibodies may lead to thrombosis and recurrent fetal loss.
Central nervous system (CNS): headaches, depression, anxiety, seizures, stroke, and cognitive impairment.
Renal system: reduced kidney function, proteinuria, and elevated serum creatinine. About 50% of SLE patients develop lupus nephritis, which is a major cause of illness and death and may progress to end-stage renal disease. The kidney damage in SLE is caused by autoantibody–immune complex deposition, leading to inflammation and infiltration by T cells, macrophages, and other immune cells.
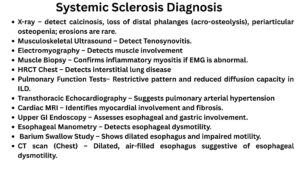
DIAGNOSIS
Diagnosing lupus is difficult because it can present with many different signs and symptoms. The disease may involve multiple organ systems, including the kidneys, lungs, skin, nervous system, and musculoskeletal system, as well as other parts of the body.
The diagnosis of SLE is made by combining clinical findings (the patient’s signs and symptoms) with laboratory test results and other diagnostic investigations.
ANA testing in SLE
Antinuclear antibodies (ANAs) are autoantibodies that attack components inside the cell nucleus. Detecting ANAs is essential for diagnosing SLE, and many patients test positive for more than one type of ANA.
Anti–double-stranded DNA (anti-dsDNA) antibodies are highly specific for SLE and are commonly associated with kidney (lupus nephritis) and skin involvement.
ANAs may also react with single-stranded DNA (ssDNA) and RNA.
Anti-Ro and anti-La antibodies are important clinically because, if present during pregnancy, they are linked to fetal heart damage (neonatal lupus).
Anti-Smith (anti-Sm) antibodies are another specific marker for SLE and are often associated with renal disease.
Other autoantibodies
Another group of autoantibodies in SLE targets phospholipids, such as cardiolipin and components of the prothrombin activator complex.
These antiphospholipid antibodies increase the risk of abnormal blood clotting (thrombosis) and pregnancy loss.
Complete blood count
A complete blood count (CBC) with differential evaluates blood cell abnormalities such as anemia, leukopenia, or thrombocytopenia.
Complete metabolic profile
A complete metabolic profile assesses organ function, particularly the liver and kidneys.
Urinalysis
Urinalysis is performed to check kidney involvement, including creatinine clearance, proteinuria, and active urinary sediment.
Complement levels measurment
Measurement of complement levels (C3 and C4) is useful because low levels may indicate active disease or disease flares, and their role continues to be studied.
Diagnostic testing is often tailored to the individual patient, depending on the organs involved:
Other diagnosis methods are
Radiography to evaluate joint involvement
Renal ultrasound to assess kidney size and damage
Chest X-ray to evaluate lung involvement
Electrocardiography (ECG) to investigate chest pain or cardiac involvement
Related article:
Osteoarthritis: Symptoms, Causes & Risk Factors
References:
Maidhof, William, and Olga Hilas. “Lupus: an overview of the disease and management options.” Pharmacy and Therapeutics 37.4 (2012): 240.